
About Peyronie’s Disease
Peyronie’s disease is an acquired physical deformity of the penis. It is most often caused by scar tissue (which we call “plaque”) in the fibrous coating of the penile erectile bodies that causes a curvature or a constriction of erections. It is a psychologically traumatic condition that lowers men’s self-esteem, inhibits normal sexual function and frequently stresses relationships. There is not always a direct cause for Peyronie’s, though it is believed to be caused by repetitive micro-trauma to the semi-erect penis, essentially a “wear-and-tear” phenomenon over time. Only about 10-15% of men will remember a physically traumatic sexual experience that caused the penis to bend forcibly and often painfully. Some people are genetically predisposed to the condition. Francois Gigot de la Peyronie was a court physician for King Louis XV of France in the 1700s. He first wrote about the condition and as such, it has carried his name for the last 300 years.
90%
Success rate with advanced treatments like Xiaflex®.
80%
Significant improvement with personalized care.
Symptoms of Peyronie’s Disease
With Peyronie’s Disease, most men will notice one or more of the following:

visible bend or curve
Most often up, but also can be left, right, or down

penis shortening
and length loss

Hourglass deformity
Narrowing of the penis at the site of plaque

Hinge Defect
The penis is weak and bends easily at the plaque

penis narrowing
at the plaque, and decreased girth past the plaque

pain during erection
or during intercourse
Diagnosing Peyronie’s Disease
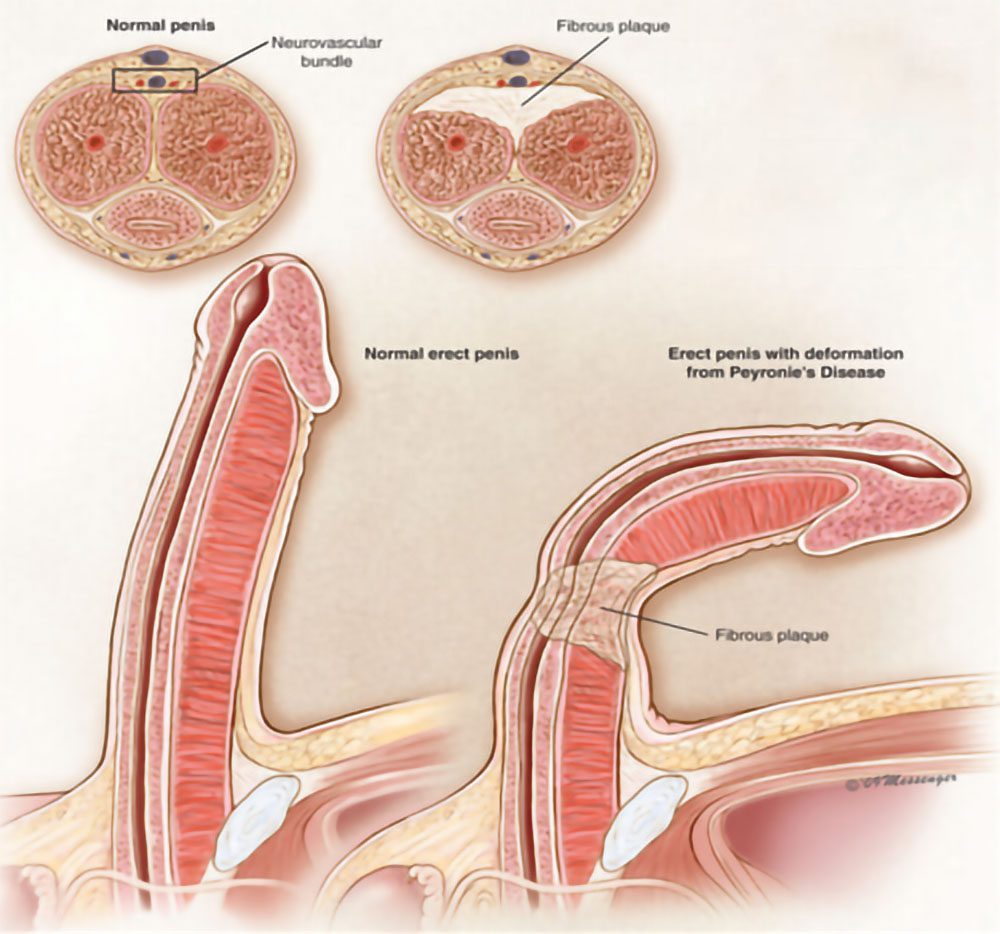
The analogy that I often use is that of a long balloon – the kind that you fold into balloon animals. Normally when you blow it up, it’s straight. Now imagine a big piece of tape slapped on one side – what happens when you blow up the balloon now? It will bend towards the side with the tape because that side can’t expand anymore. It will also constrict it’s length-wise expansion. That’s essentially what’s happening in Peyronie’s – the penis is the balloon, and the plaque is the piece of tape.
The patient usually makes the diagnosis of Peyronie’s when he notices his penis develops a curve with erections. Some men will develop severe curvature overnight, others will take months to develop the deformity. It can be painful, especially in the first few months of development. Specialists divide PD into 2 categories: acute and chronic. The acute phase can last up to a couple of years but most men evolve into the chronic phase in the first 6-12 months after noticing the curvature. Along with curvature, most men will notice loss of penile length which can sometimes be dramatic. Some men claim losing up to ½ of their former erect penis length. Penile shortening occurs because the thick fibers of the penis are usually elastic and stretch with blood flow, but the plaque prevents the tissue from stretching, and men find themselves with a smaller erect penis. Talk about adding insult to injury.
As with most things in medicine, there are a few general options, which I divide into categories. I use this mnemonic a lot, and it applies to both Peyronie’s and ED.

Treatment Options for Peyronie’s Disease
One important thing to consider is what the treatment goals for a man with Peyronie’s are. If ever a surgeon tells you that they can give you back the penis you had when you were 18, you should run in the other direction, because that is simply not possible. What then, are reasonable treatment goals? We will set these together, but generally, what we are aiming for is a rigid, reliable, physiologically straight (usually meaning 5-10 degrees or less), penetrative penis that can be used to have intercourse without pain. That’s really the goal, isn’t it?